As a physics reporter and lover of mathematics, I won’t be celebrating Pi Day this year. That’s because pi is wrong.
I don’t mean that the value is incorrect. Pi, known by the symbol π, is the number you get when you divide a circle’s circumference by its diameter: 3.14159… and so on without end. But, as some mathematicians have argued, the mathematical constant was poorly chosen, and students worldwide continue to suffer as a result.
A longtime fixture of high school math classes, pi has inspired books, art (SN Online: 5/4/06) and enthusiasts who memorize it to tens of thousands of decimal places (SN: 4/7/12, p. 12). But some contend that replacing pi with a different mathematical constant could make trigonometry and other math subjects easier to learn. These critics — including myself — advocate for an arguably more elegant number equal to 2π: 6.28318…. Sometimes known as tau, or the symbol τ, the quantity is equal to a circle’s circumference divided by its radius, not its diameter.
This idea is not new. In 2001, mathematician Bob Palais of the University of Utah in Salt Lake City published an article in the Mathematical Intelligencer titled “ π is wrong!” The topic gained more attention in 2010 with The Tau Manifesto, posted online by author and educator Michael Hartl. But the debate tends to reignite every year on March 14, which is celebrated as Pi Day for its digits: 3/14. The simplest way to see the failure of pi is to consider angles, which in mathematics are typically measured in radians. Pi is the number of radians in half a circle, not a whole circle. That makes things confusing: For example, the angle at the tip of a slice of pizza — an eighth of a pie — isn’t π/8, but π/4. In contrast, using tau, the pizza-slice angle is simply τ/8. Put another way, tau is the number of radians in a full circle.
That factor of two is a big deal. Trigonometry — the study of the angles and lines found in shapes such as triangles — can be a confusing whirlwind for students, full of blindly plugging numbers into calculators. That’s especially true when it comes to sine and cosine, two important functions in trigonometry. Many trigonometry problems involve calculating the sine or cosine of an angle. When graphed, the two functions look like a series of wiggles, shaped a bit like an “S” on its side, that repeat the same values every 2π. That means pi covers only half of an S. Tau, on the other hand, covers the full wiggle, a more intuitive measure.
Pi has become so embedded in mathematics that it could be hard to excise. A more practical approach may be to introduce tau as a teaching tool alongside pi, rather than a replacement. Education is where tau’s impact is most likely to be felt: Professional scientists and mathematicians can comfortably handle the factors of two that crop up with pi in equations.
You might argue that multiplying by two isn’t that hard, even for students. But it isn’t the arithmetic that concerns me. Trigonometry is notorious for creating a divide between the math-fluent and math-phobic. But helping more people understand and enjoy mathematics isn’t some pie-in-the-sky fantasy. Everyone is capable of doing math. We just need to work smarter, and speak more clearly, to help those who struggle.
BOSTON — The bond between parent and child is powerful enough to override fear. New research shows that if a parent sits with a young child during a potentially scary situation, the child isn’t as afraid of it later.
The study is in line with research suggesting that during particular stages of development, a strong connection with a caregiver tamps down activity in the amygdala, the brain structure that helps process fear and spurs the fight-or-flight response. “Fight or flight is pointless if you are tiny,” said developmental neuroscientist Nim Tottenham of Columbia University, who presented the work March 26 at a Cognitive Neuroscience Society meeting. For young kids, the bond with a caregiver not only helps ensure survival but also makes kids feel safe, enabling them to approach the world with confidence, Tottenham said. “Attachment is a strategy that has worked very well; it trumps everything.”
Kids from ages 3 to 5 were shown two shapes — a green triangle and a blue square. Just the square was accompanied by a loud, fingers-on-the-chalkboard kind of noise. Some kids had a parent sitting next to them while they saw the shapes; others sat with a researcher. After the parents left, kids chose which door to go through to get a present: one with the scary blue square on it, the other with the innocuous green triangle.
Kids paired with the experimenter avoided the door with the blue square. But kids who had sat next to a parent showed a slight preference for that door, even though they knew they would collect the same present from behind either door.
Stephen Hawking, a black hole whisperer who divined the secrets of the universe’s most inscrutable objects, left a legacy of cosmological puzzles sparked by his work, and inspired a generation of scientists who grew up reading his books.
Upon Hawking’s death on March 14 at age 76, his most famous discovery — that black holes aren’t entirely black, but emit faint radiation — was still fueling debate.
Hawking “really, really cared about the truth, and trying to find it,” says physicist Andrew Strominger of Harvard University, who collaborated with the famed scientist. Hawking “was deeply committed, his whole life, to this quest of understanding more about the physical universe around us.”
After earning his Ph.D. in 1965 at the University of Cambridge, Hawking continued studying cosmology there for the rest of his life. Due to a degenerative illness, amyotrophic lateral sclerosis, or ALS, Hawking gradually lost control of his body, requiring a wheelchair and eventually a voice synthesizer to speak. Yet his desire to uncover nature’s secrets remained boundless. In one of the most significant realizations of his career, Hawking reported in 1974 that black holes emit a faint glow of particles. This effect arises from quantum mechanics, which states that a sea of transient particles and antiparticles pervades all of space. These “virtual” particles usually annihilate in an instant, but if one of those particles is lost inside a black hole’s boundary, or event horizon, its partner can escape, producing what’s now known as Hawking radiation (SN: 5/31/14, p. 16).
As a result, black holes can gradually evaporate and disappear. This led to a still unresolved paradox: Throw an encyclopedia into a black hole and the information will eventually be lost. But according to quantum mechanics, information can never be destroyed.
Many solutions have been proposed for this problem, but none has stuck. In 2016, Hawking and colleagues proposed a path toward a solution: Black holes might have “soft hair,” low-energy particles that would retain information about what fell inside (SN: 2/06/16, p. 16). Hawking’s collaborators, including Strominger, are still working on the research. Standing at the interface between two seemingly incompatible theories — quantum mechanics, which describes the very small, and the general theory of relativity, which describes gravity — the quandary and its resolution may eventually help reveal a unified theory of quantum gravity.
Hawking made many other contributions, including studies of spacetime curvature during the Big Bang and the possibility that mini black holes might have formed in the universe’s infancy. Despite their groundbreaking nature, Hawking’s ideas remained largely theoretical, says Harvard theoretical astrophysicist Avi Loeb. Hawking radiation, for example, has never been directly detected. “That’s, unfortunately, why he didn’t get the Nobel Prize,” Loeb says. Yet Hawking achieved a level of fame uncommon among scientists. He excelled at making abstruse science digestible to the public. With his books, most notably the best-selling A Brief History of Time, first published in 1988, Hawking inspired countless future scientists and science lovers (including the author of this article). Theoretical cosmologist Katie Mack of North Carolina State University in Raleigh first opened the book when she was about 10 years old. “I found it so fascinating at the time,” she says. “I found out that Stephen Hawking was called a cosmologist and so I said I wanted to be a cosmologist.” Hawking similarly motivated dozens of her colleagues, Mack says.
Hawking remained active in research even in the last months of his life. A paper on which he is a coauthor, which was updated in the weeks before his death, considered the physics of multiverses, the possibility that a slew of other universes exist in addition to our own.
A funeral was held for Hawking on March 31. Later this year, his ashes will be interred in Westminster Abbey in London, where they will rest alongside the remains of other famous British scientists, including Isaac Newton and Charles Darwin.
While the data was amassing, suddenly there came a tapping, As of something gently rapping, rapping at LIGO’s door.
The source of a mysterious glitch in data from a gravitational wave detector has been unmasked: rap-tap-tapping ravens with a thirst for shaved ice. At the Advanced Laser Interferometer Gravitational-Wave Observatory, or LIGO, in the desert of Hanford, Wash., scientists noticed a signal that didn’t look like gravitational waves, physicist Beverly Berger said on April 16 at a meeting of the American Physical Society.
A microphone sensor that monitors LIGO’s surroundings caught the sounds of pecking birds on tape in July 2017, Berger, of the LIGO Laboratory at Caltech, said. So the crew went out to the end of one of the detector’s 4-kilometer-long arms to check for evidence of the ebony birds at the scene.
Sure enough, frost covering a pipe connected to the cooling system was covered in telltale peck marks from the thirsty birds. One raven, presumably seeking relief from the desert heat, was caught in the act. Altering the setup to prevent ice buildup now keeps the ravens from tapping, evermore.
After a two-day delay, the planet-hunting TESS telescope successfully launched into a clear blue sky at Cape Canaveral, Fla., at 6:51 p.m. EDT on April 18.
TESS, the Transiting Exoplanet Survey Satellite, is headed to an orbit between the Earth and the moon, a journey that will take about two months. In its first two years, the telescope will seek planets orbiting 200,000 nearby, bright stars, and identify the best planets for further study. TESS’ cameras will survey 85 percent of the sky by splitting it up into 26 zones and focusing on each zone for 27 days apiece.
TESS launched on a SpaceX Falcon 9 rocket. A previous launch attempt on April 16 was scrubbed so that SpaceX could run more tests on the rocket’s guidance, navigation and control system. SpaceX recovered the rocket’s first stage booster on an autonomous drone ship and hopes to reuse the rocket on a future launch.
Quantum entanglement has left the realm of the utterly minuscule, and crossed over to the just plain small. Two teams of researchers report that they have generated ethereal quantum linkages, or entanglement, between pairs of jiggling objects visible with a magnifying glass or even the naked eye — if you have keen vision.
Physicist Mika Sillanpää and colleagues entangled the motion of two vibrating aluminum sheets, each 15 micrometers in diameter — a few times the thickness of spider silk. And physicist Sungkun Hong and colleagues performed a similar feat with 15-micrometer-long beams made of silicon, which expand and contract in width in a section of the beam. Both teams report their results in the April 26 Nature. “It’s a first demonstration of entanglement over these artificial mechanical systems,” says Hong, of the University of Vienna. Previously, scientists had entangled vibrations in two diamonds that were macroscopic, meaning they were visible (or nearly visible) to the naked eye. But this is the first time entanglement has been seen in macroscopic structures constructed by humans, which can be designed to meet particular technological requirements.
Entanglement is a strange feature of quantum mechanics, through which two objects’ properties become intertwined. Measuring the properties of one object immediately reveals the state of the other, even though the duo may be separated by a large distance (SN: 8/5/17, p. 14).
Quantum mechanics’ weird rules typically apply to small fry — atoms, electrons and other tiny particles — and not to larger things such as cats, chairs or buildings. But that division leads to a confounding puzzle. “Atoms behave like atoms, and cats behave like cats, and so where is that transition in between?” says physicist Ben Sussman of the National Research Council of Canada in Ottawa, who was not involved in the research.
Now, scientists are extending the dividing line to larger and larger objects. “One of our motivations is to keep on testing how far we can push quantum mechanics,” says Sillanpää, of Aalto University in Finland. “There might be some fundamental limit for how big objects can be” and still be quantum. In Sillanpää’s experiment, two tiny aluminum sheets — consisting of about a trillion atoms and just barely visible with the naked eye — vibrate like drumheads and interact with microwaves bouncing back and forth in a cavity. Those microwaves play the role of drum major, causing the two drumheads to sync up their motions. In many previous demonstrations of entanglement, the delicate quantum link is transient. But this one was long-lived, persisting as long as half an hour in experiments, Sillanpää says, and, in theory, even longer. “Our entanglement lasts forever, basically.” Taking a different tactic, Hong and colleagues demonstrated entanglement with two silicon beams, big enough to be seen with a magnifying glass. Within a region of each beam, in a 1-micrometer-long section composed of about 10 billion atoms, the structure expanded and contracted — as if taking deep breaths in and out — in response to being hit with light. Instead of microwaves, Hong and colleagues’ work used infrared light of the wavelength typically transmitted in telecommunications networks made of optical fibers, which means it could be incorporated into a future quantum internet. “From a technology standpoint, that really is crucial,” says physicist John Teufel of the National Institute of Standards and Technology in Boulder, Colo., who was not involved with the work.
Scientists could use such vibrating structures within a quantum network to convert quantum information from one type to another, transitioning from particles of light to vibrations, for example. Once constructed, a quantum internet could allow quantum computers to communicate and provide unhackable communication across the globe (SN: 10/15/16, p. 13).
The ability to entangle these specially designed structures moves scientists a step closer to that vision. “You can really start to think about building real devices with these things,” Sussman says.
New insights into how stars like the sun die might help explain why astronomers find bright planetary nebulae where they’re least expected. Simulations of how these stellar remnants form suggest that smaller stars have cores that heat up fast enough to produce bright nebulae upon their demise, researchers report online May 7 in Nature Astronomy.
A planetary nebula is what’s left over when a sunlike star sheds its outer envelope of gas. Radiation from the stellar core, now exposed, sets the expanding shell of gas aglow, creating the kind of candy-colored clouds seen in spectacular Hubble Space Telescope images, like that of the Cat’s Eye Nebula and the butterfly-shaped NGC 6302 (SN Online: 9/5/13). Astronomers had thought a star’s mass dictated what sort of nebula it produced, with more massive stars creating the brightest nebulae and stars with lower masses, like the sun, making nebulae too faint to see from another galaxy.
But that idea didn’t match observations: The brightest planetary nebulae in older elliptical galaxies — thought to be home to only low-mass stars — are just as luminous as those in younger, spiral galaxies, where massive stars abound. The puzzle vexed astronomers for decades.
Now, astrophysicist Albert Zijlstra at the University of Manchester in England, and colleagues have simulated planetary nebulae formation based on a new theory of stellar evolution. This theory says that after smaller stars shed their outer envelopes, their bare cores heat up more quickly than previously thought. That allows the cinderlike stellar core to pump more energetic radiation into the surrounding nebula before the gas expands too far out into space, ultimately making for a brighter nebula, explains Christophe Morisset, an astronomer at the National Autonomous University of Mexico in Mexico City not involved in the work.
Simulations showed that stars ranging from 1.1 to three times the mass of the sun produce nebulae with similar brightness. That result could explain why nebulae found in galaxies with stars that are 7 billion years old can be just as bright as those found in galaxies chock-full of 1-billion-year-old stars. This finding marks “an important step forward” in understanding the universe’s population of planetary nebulae, says Penn State astronomer Robin Ciardullo, who was not involved in the work.
But some mystery still remains: For the most ancient elliptical galaxies with very small stars over 7 billion years old, the simulations didn’t produce planetary nebulae bright enough to match what astronomers see in the sky. So there’s still “a little ways to go” before astronomers can explain why bright nebulae are so ubiquitous, he says.
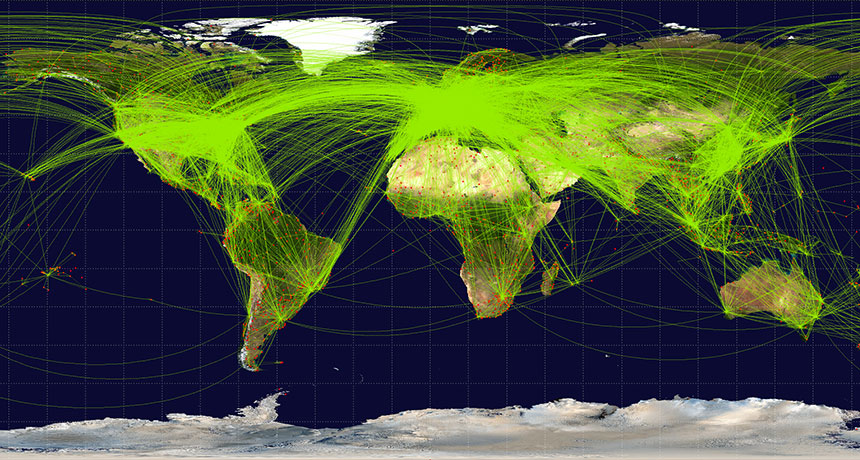
Global tourism contributes about 8 percent of total greenhouse gas emissions to the atmosphere, researchers report May 7 in Nature Climate Change. That carbon footprint is about three times as large as tourism-related emissions estimated by previous studies.
The jump is largely because the new study doesn’t just tally up emissions from the traveling itself, like hopping a flight, going on a road trip or taking a cruise. It also looks at the impact of the goods and services that tourists enjoy, from food to shopping to hotel stays. Who has the biggest carbon footprint? The United States topped the list, as both a top destination for tourists and a source of tourists. Other prosperous nations, such as Canada and Germany, also have a big footprint, and increasingly wealthy nations, such as China and Mexico, are catching up in this amazing race.
Take a look at global tourism by the numbers:
4.5 gigatons The amount of carbon dioxide and other greenhouse gases that came from tourism in 2013.
2.7 percent The share of the global total of emissions that comes just from Canadians and Mexicans traveling to the United States for tourism.
300 kilograms Increase, from 2009 to 2013, in the yearly carbon footprint for each inhabitant of the tiny island nation of the Maldives as a result of international tourism.
$4.7 trillion The amount of money, in U.S. dollars, spent on global tourism in 2013. That’s up from $2.5 trillion in 2009.
3 percent Current annual growth in money spent on global tourism, which translates to tourism-related emissions of 6.5 gigatons of carbon dioxide and other greenhouse gases by 2025.
It’s vacation season — time for swimming pools, hot tubs and water parks. But you might want to think twice before getting wet, says a new report from the U.S. Centers for Disease Control and Prevention.
From 2000 to 2014, public health officials from 46 states and Puerto Rico reported 493 outbreaks associated with treated recreational water, resulting in more than 27,000 illnesses and eight deaths, according to a report in the May 18 Morbidity and Mortality Weekly Report. Hotel pools and hot tubs were the setting for about a third (32 percent) of the outbreaks, followed by public parks (23 percent), club/recreational facilities (14 percent) and water parks (11 percent).
Most of the infections were from three organisms that can survive chlorine and other commonly used disinfectants: Cryptosporidium, a parasite that can cause gastrointestinal problems; Pseudomonas, a bacteria that causes swimmer’s ear; and Legionella, a bacteria that causes a pneumonia-like illness.
So, what to do? The CDC recommends a few steps before diving in: Don’t swallow pool water. Don’t let children with diarrhea in the water. And use test strips to measure levels of pH, bromine and chlorine in the water. The cleaner the water, the safer to swim.
When severe, chronic diarrhea strikes, sometimes the only cure is … more feces. It might seem bizarre, but a transplant of healthy human stool and its bacterial ecosystem can mean freedom from a painful, life-threatening illness.
The transplants — called fecal microbiota transplants, or FMTs — are becoming more and more popular. So popular that the stool bank OpenBiome has supplied more than 30,000 stool samples to clinicians and scientists since 2012. Right now, though, the government isn’t quite sure how to regulate fecal transplants. That uncertainty comes from what seems like a simple question: What is poop? Is it a drug? Is it a bodily tissue? Is it a little of both? Then, is the transplant itself a procedure? That’s a whole other regulatory category.
Out of concern that regulations would cut out desperate patients or send companies running to more profitable enterprises, some FMTs aren’t actually regulated at all. That leads to the potential for unscreened and potentially dangerous fecal samples to flood the market. A group of doctors and scientists from the University of Maryland School of Medicine in Baltimore have tried to cut through the confusion with a three-track policy plan that would help keep poop transplants clean (as clean as fecal matter gets, anyway), while still allowing patients to get transplants when they need them. The scientists also hope to encourage companies to develop potentially lucrative products for future FMTs — including options that are almost feces-free.
A fecal transplant involves taking a mixture of a donor’s poop and saline (sometimes mixed with the help of a kitchen blender) and inserting it into a patient’s large intestine or far down the gut with a nasogastric tube. Companies are working on alternatives to that procedure, such as pills that deliver the same benefits with less of an “ick” factor. Currently, FMTs have the most potential for treating Clostridium difficile infections. C. diff is a bacterium normally found in our guts and feces. But unchecked, it can take over the large intestine. The result is inflammation and chronic severe diarrhea that can last weeks or months. There are more than 450,000 estimated cases in the United States each year, and more than 29,000 deaths. Doctors can prescribe antibiotics to kick the bugs out, but in 20 percent of patients, the infection comes back again. And again.
For those patients, FMTs can be a miracle. They resolve symptoms in 85 percent of patients with recurrent C. diff infections, compared with the roughly 20 to 30 percent success rates of antibiotics.
Unfortunately, FMTs also come with a dose of danger. Feces is a mixture of our undigested waste, the beneficial microbes needed to keep our guts healthy and whatever bacteria, fungi and viruses we’ve picked up in our busy lives. So donors need to be screened for pathogens that might make a sick recipient sicker. And the poop needs to be handled carefully to avoid contamination or infection in the people who handle and receive it.
Gastroenterologist Erik von Rosenvinge of the University of Maryland School of Medicine in Baltimore has performed more than 40 FMTs. “When I first started doing these in 2013, I was having the patients identify a friend or family member, and they would bring in the stool and I would process it myself,” he says. After the first few donations, von Rosenvinge switched to using stool from the OpenBiome stool bank. It saves money and time.
For each donation, the stool bank or hospital will test the feces for pathogens. But who sets the standard to ensure that people getting treated for C. diff are receiving “clean” stool, either from their friends or from a stool bank?
Well, right now, no one.
Poop: Drug or tissue? The first problem is to figure out what an FMT actually is, at least, in terms of how the government should regulate one. Feces is like a drug, in that the microbes in it can change how the body functions. But because of those very microbes, feces is also a living thing that differs from person to person. In fact, in some ways, poop is like biological tissue, in that it comes from the human body.
But then, the FMT itself is something like a procedure — there’s a method involved in getting one. But that procedure is also delivering a drug. Or is it transplanting a tissue? Here we go again.
“The FDA has been reticent to create a new regulatory product category,” says Jacques Ravel, who studies the microbiome and women’s health at the University of Maryland School of Medicine. “They’ve been trying to fit the stool into one of the regulated product categories, and there’s limitations every time you do, there’s pros and cons.”
In 2013, the FDA declared that FMTs counted as a drug (technically a “live biotherapeutic product”) in terms of how they would be regulated, which, von Rosenvinge notes, “means all of us are pharmaceutical factories,” pooping out “drugs” once a day on average.
But FMTs don’t have FDA approval yet, so as a drug, an FMT is considered “investigational.” Giving one to a patient would require an investigational new drug application, or IND. Those are associated with clinical trials, meaning someone who needed an FMT would probably have to get into a clinical trial to get treatment. “At that point [in 2013], I’d only done a handful, and I had to stop because I didn’t have an IND,” von Rosenvinge recalls.
The FDA’s goal was to make sure that FMTs were safe for people. But the requirements meant that most doctors could not give FMTs. At a public workshop about FMTs in 2013, scientists and physicians spoke out against the requirements. In response, the FDA noted that it would practice “enforcement discretion.” That’s government-speak for politely looking the other way while doctors treated C. diff patients outside of clinical trials.
Unfortunately, looking the other way means that FMTs — whether prepared from a donor by a doctor or purchased from a stool bank — are still completely unregulated. As FMTs gain popularity for C. diff, von Rosenvinge notes, that could lead to problems. “You don’t want someone grabbing poop out of the local [port-a-potty] and selling it. That would be horrible,” he says. “If someone’s going to be using stool to put into a human, you want to have assurances that it was properly handled, that the donor was properly screened, that we’re doing everything within reason to minimize risk of causing problems.”
The stool banks themselves aren’t pleased with the arrangement, either. “We’re all operating on a bit of uncertainty,” says Carolyn Edelstein, the executive director of OpenBiome. Right now, OpenBiome screens all of their samples by their own standards, because the government hasn’t given them any. Everyone knows that “looking the other way” could end at any time, a move that the FDA proposed in March 2016. Then, INDs would be required again, and patients could be out of luck.
Balancing regulation and access To patients, access — cheap access — is paramount. “The big challenge at the end of the day is access to treatment, and the fact that FMT is really cheap as its performed right now,” says Ravel. “Right now there’s no true alternative, even those coming down the pipe may be able to cure [C. diff], but they’re not going to be cheap.”
But to doctors, scientists and government, access needs to be balanced with safety. “People are doing this at home, and I think that raises issues about the safety of donations,” notes Diane Hoffman, who studies health law at the University of Maryland. “Do [patients] understand the potential for contamination and disease transmission?”
The right balance might also help promote the development of new drugs for treating C. diff — ones that extract the most useful bacteria, for example, and don’t involve an enema.
To this end, Hoffman, von Rosenvinge, Ravel and colleagues worked with a large working group of scientists, lawyers, industry partners and patient advocates to come up with recommendations for regulating FMTs, which they outlined in December in Science. The result is a slim, three-track system.
Individual FMTs for C. diff done by doctors with donors who are friends or family of the patients would be classified under “practice of medicine.” This is an exception that allows doctors to use their expertise and judgment when treating patients, as long as the treatments they’re using are legally available. No FDA approval or IND required. “We’re trusting the doctor to do what’s in the best interests of the patient,” Hoffman explains.
Stool banks, on the other hand, would be regulated like tissue banks. They’d have to comply with good manufacturing and safety practices and screen and test their donors. The banks would also have to track the patients who receive donations, and submit their long-term data to a national registry. The banks would be free to sell FMT samples, but only to treat C. diff. Any other use that the FMT hasn’t been approved for would still require a clinical trial.
The third track would be for “stool-based products.” These would be pills or delivery systems that offer, say, combinations of microbes, rather than the current practice of basically “polishing a turd,” notes von Rosenvinge. These would be regulated as biological products or drugs.
In practice, this would mean stool banks and stool transplants would be regulated more like cell and tissue banks and transplants. “Stool-based products” on the other hand, would be regulated more like drugs. No matter what, patients would have to be informed of all the risks associated with an FMT. “I think the stand-out, excellent point of this proposed regulatory scheme is that stool banks need to be regulated, and there need to be rigorous data collection of outcomes,” says Kelly Hills, a bioethicist with Rogue Bioethics. “Track everything. The whole enchilada. We have historical precedents [such as in vitro fertilization] where we didn’t track outcomes, and 20 or 40 years down the line we’ve been kicking ourselves. It’d be nice to learn from our mistakes!”
This is especially important because while FMTs have very clear benefits for C. diff in the short term, no one really knows what the long-term effects will be. “We don’t have a lot of [long-term data] right now,” Hills notes. “We know that when you change someone’s gut microbiome you actually change a lot in their life. We have the anecdotal stories of people losing lots of weight, for example, or people’s dietary desires changing.” But the plural of anecdote isn’t data. A registry might help scientists keep track of exactly what transplants people received and their long-term effects.
But “practice of medicine” might give too much leeway to doctors to try FMT for things that they probably shouldn’t, worries Leigh Turner, a bioethicist at the University of Minnesota in Minneapolis. “‘Practice of medicine’ isn’t a curb on advertising or promotional claims,” he notes.
The group behind the policy proposal was careful not to stand in the way of further drug development. That third track was designed with the hope of promoting stool-based products, so that companies might be encouraged to pursue more of them. But if FMTs aren’t broken, why would companies — let alone patients — want to take the risks to fix them? With FMTs freely available, it might be hard to recruit patients to potential clinical trials for new drugs. “If you have a cheap solution that works and you have a patient with C. diff, that patient will not want to enter a trial with a placebo arm,” notes Ravel. After all, what if they got the placebo? They want a cure, not a game of roulette.
The policy brief isn’t policy, and the FDA hasn’t made a final call. But looking the other way isn’t going to cut it in the long term. FMTs are only used for recurrent C. diff infections right now. But scientists are interested in them for many other things. “You can get into weird science fiction areas. Would athletes start doing FMTs to try and improve their Tour de France time? Could you lose weight?” notes Hills. Some of these could be lucrative options for companies. And because FMTs are so easy to perform, people are already making headlines with the do-it-yourself route.
No matter what, a lack of regulation isn’t a long-term strategy. People are going to find other uses for feces, and the FDA will need to be prepared when they do.