In a hotel ballroom in Seoul, South Korea, early in 2016, a centuries-old strategy game offered a glimpse into the fantastic future of computing.
The computer program AlphaGo bested a world champion player at the Chinese board game Go, four games to one (SN Online: 3/15/16). The victory shocked Go players and computer gurus alike. “It happened much faster than people expected,” says Stuart Russell, a computer scientist at the University of California, Berkeley. “A year before the match, people were saying that it would take another 10 years for us to reach this point.” The match was a powerful demonstration of the potential of computers that can learn from experience. Elements of artificial intelligence are already a reality, from medical diagnostics to self-driving cars (SN Online: 6/23/16), and computer programs can even find the fastest routes through the London Underground. “We don’t know what the limits are,” Russell says. “I’d say there’s at least a decade of work just finding out the things we can do with this technology.”
AlphaGo’s design mimics the way human brains tackle problems and allows the program to fine-tune itself based on new experiences. The system was trained using 30 million positions from 160,000 games of Go played by human experts. AlphaGo’s creators at Google DeepMind honed the software even further by having it play games against slightly altered versions of itself, a sort of digital “survival of the fittest.”
These learning experiences allowed AlphaGo to more efficiently sweat over its next move. Programs aimed at simpler games play out every single hypothetical game that could result from each available choice in a branching pattern — a brute-force approach to computing. But this technique becomes impractical for more complex games such as chess, so many chess-playing programs sample only a smaller subset of possible outcomes. That was true of Deep Blue, the computer that beat chess master Garry Kasparov in 1997.
But Go offers players many more choices than chess does. A full-sized Go board includes 361 playing spaces (compared with chess’ 64), often has various “battles” taking place across the board simultaneously and can last for more moves.
AlphaGo overcomes Go’s sheer complexity by drawing on its own developing knowledge to choose which moves to evaluate. This intelligent selection led to the program’s surprising triumph, says computer scientist Jonathan Schaeffer of the University of Alberta in Canada. “A lot of people have put enormous effort into making small, incremental progress,” says Schaeffer, who led the development of the first computer program to achieve perfect play of checkers. “Then the AlphaGo team came along and, incremental progress be damned, made this giant leap forward.”
Real-world problems have complexities far exceeding those of chess or Go, but the winning strategies demonstrated in 2016 could be game changers.
Drug use continued to threaten the health and safety of the American public in 2016, while a hidden menace in drinking water remained a major worry for the people of Flint, Mich.
Teen vaping Vaping has surpassed cigarette smoking among U.S. high school students, according to a report released in 2016 from the National Youth Tobacco Survey. Estimates suggest that some 2.39 million U.S. high school kids vaped in 2015, compared with an estimated 1.37 million who smoked cigarettes (SN: 5/28/16, p. 4). The popularity of e-cigarettes has increased recently despite a lack of evidence showing that they are safer than conventional tobacco products, according to the U.S. Food and Drug Administration, which in May extended its regulatory authority to e-cigarettes. Studies reported in 2016 show a host of potential health risks, including effects on the brain, immune system and fertility (SN: 3/5/16, p. 16). Opioid epidemic Against a backdrop of rising prescription opioid addiction, deaths related to opioid use have become an issue of national importance. A surge in fentanyl-spiked drugs emerged as a primary concern in 2016 (SN: 9/3/16, p. 14). U.S. deaths from synthetic opioids rose from 3,105 in 2013 to 5,544 in 2014, a change that could not be explained by fentanyl prescription rates, according to a report released in August by the Centers for Disease Control and Prevention. Drug enforcement seizures involving fentanyl more than doubled from 2014 to 2015.
Fallout in Flint After lead in the drinking water in Flint, Mich., launched a public health crisis (SN: 3/19/16, p. 8), a federal state of emergency remained in effect into August. The most recent tests conducted by the U.S. Environmental Protection Agency show that levels of lead, which is toxic to the brain, are below those considered dangerous and that filtered tap water is safe to drink. Many residents are still relying on bottled water, however. There’s also growing concern that lead contamination and testing is not being taken seriously elsewhere in the United States.
The moon is made of moons, new simulations suggest. Instead of a single colossal collision forming Earth’s cosmic companion, researchers propose that a series of medium to large impacts created mini moons that eventually coalesced to form one giant moon.
This mini-moon amalgamation explains why the moon has an Earthlike chemical makeup, the researchers propose January 9 in Nature Geoscience.
“I think this is a real contender in with the other moon-forming scenarios,” says Robin Canup, a planetary scientist at the Southwest Research Institute in Boulder, Colo., who was not involved in the new work. “This out-of-the-box idea isn’t any less probable — and it might be more probable — than the other existing scenarios.” A collision between Earth and a Mars-sized object called Theia around 4.5 billion years ago is the current leading candidate for how the moon formed. This impact would have been a glancing blow rather than a dead-on collision, with most of the resulting building materials for the moon coming from Theia. But the moon and Earth are compositional dead ringers for one another, casting doubts on a mostly extraterrestrial origin of lunar material and thus the single impact explanation. Planetary scientist Raluca Rufu of the Weizmann Institute of Science in Rehovot, Israel, and colleagues dusted off a decades-old, largely disregarded hypothesis that the moon instead formed from multiple impacts. In this scenario, the early Earth was hit by a series of objects a hundredth to a tenth of Earth’s mass. Each impact could have created a disk of debris around Earth that assembled into a moonlet, the researchers’ simulations show. Over tens of millions of years, about 20 moonlets could have ultimately combined to form the moon. Multiple impacts help explain why Earth and the moon are chemically similar. For example, each impact may have hit Earth at a different angle, excavating more earthly material into space than a singular impact would.
The single impact hypothesis has about a 1 to 2 percent chance of yielding the right lunar mix based on the makeup of potential impactors in the solar system. In the researchers’ simulations, the multiple impact scenario is correct tens of percent of the time. Further investigation of the interiors and composition of the Earth and moon, the researchers say, should reveal whether this explanation is correct.
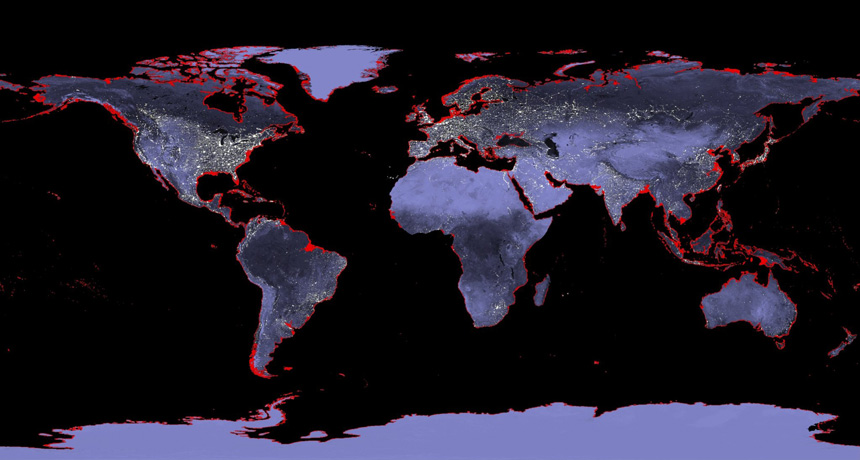
The last time Earth’s thermostat was cranked as high as it is today, sea levels were high enough to completely drown New Orleans (had it existed at the time), new research suggests.
Ocean surface temperatures around 125,000 years ago were comparable to those today, researchers report in the Jan. 20 Science. Previous estimates suggested that this period, the height of the last warm phase in the ongoing ice age, was as much as 2 degrees Celsius warmer. Climate scientists often use the last interglacial period as a reference point for predicting how rising temperatures will affect sea levels. The new results, the researchers write, will help scientists better predict how Earth’s oceans and climate will respond to modern warming. Warming 125,000 years ago raised sea levels 6 to 9 meters above present-day levels.
The global scale of that warming has been difficult to estimate. Chemical clues inside dozens of seafloor sediment samples collected from around the world provide only regional snapshots of the ancient climate. Combining 104 of these dispersed data points, climate scientist Jeremy Hoffman of Oregon State University in Corvallis and colleagues pieced together a global climate picture.
Average global sea surface temperatures around 125,000 years ago were indistinguishable from the 1995 to 2014 average, the researchers estimate.
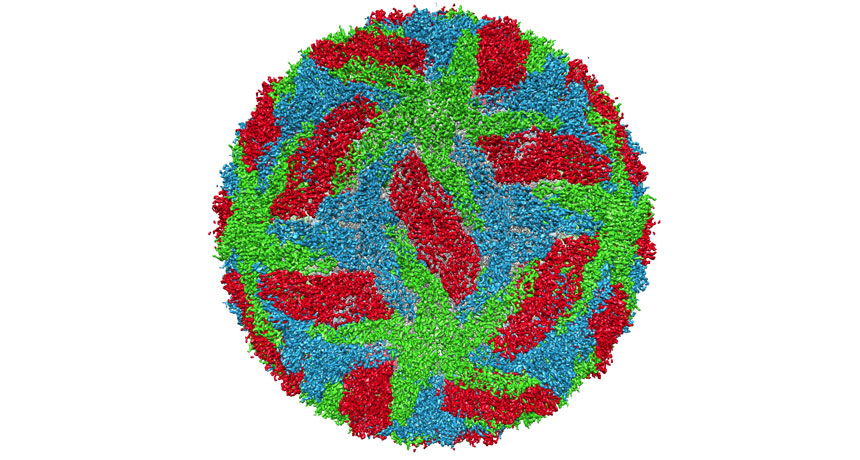
The playground ditty “first the worst, second the best” isn’t always true when it comes to dengue fever. Some patients who contract the virus a second time can experience more severe symptoms. A rogue type of antibody may be to blame, researchers report in the Jan. 27 Science. Instead of protecting their host, the antibodies are commandeered by the dengue virus to help it spread, increasing the severity of the disease.
Four closely related viruses cause dengue, a mosquito-transmitted disease marked by fever, muscle pain and other flulike symptoms. When a previously infected person contracts a second type of dengue, leftover antibodies can react with the new virus. Fewer than 15 percent of people with a second infection develop severe dengue disease. Those who do may produce a different type of antibody, says Taia Wang, an infectious diseases researcher with the Stanford University School of Medicine.
Wang and colleagues found that dengue patients with a dangerously low blood platelet count — a sign of severe dengue disease — had an abundance of these variant antibodies.
Tests in mice supported the connection. “We found that when we transferred the antibodies from patients with severe disease into mice, they triggered platelet loss,” Wang says.
Wang says it’s not known why some people have this alternate antibody. She and her team want to determine that, along with how these antibodies are regulated by the immune system. With further research, they may be able to screen people to identify those more susceptible to severe dengue disease, Wang says.
Anna Durbin, a dengue vaccine researcher at the Johns Hopkins Bloomberg School of Public Health, doesn’t see a strong connection between this type of antibody and the severity of dengue disease. But she says that the research was interesting in how it connected dengue to low platelet count, a condition known as thrombocytopenia.
“There’s a lot of different theories out there about the role of dengue antibodies and thrombocytopenia, and whether or not the virus itself can enter platelets,” Durbin says. “I think this paper may provide more insight into what is the pathogenic mechanism of thrombocytopenia and dengue, and raises some good avenues for further research.”
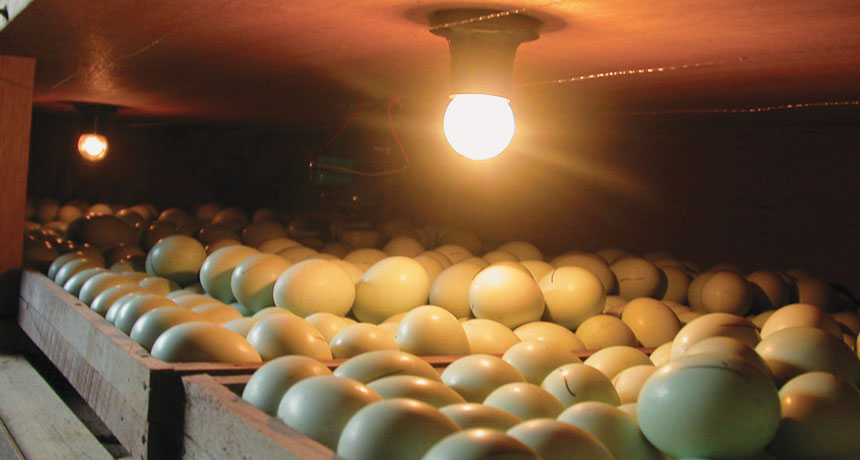
Fearful, flighty chickens raised for eating can hurt themselves while trying to avoid human handlers. But there may be a simple way to hatch calmer chicks: Shine light on the eggs for at least 12 hours a day.
Researchers at the University of California, Davis bathed eggs daily in light for different time periods during their three-week incubation. When the chickens reached 3 to 6 weeks old, the scientists tested the birds’ fear responses. In one test, 120 chickens were randomly selected from the 1,006-bird sample and placed one by one in a box with a human “predator” sitting visibly nearby. The chickens incubated in light the longest — 12 hours — made an average of 179 distress calls in three minutes, compared with 211 from birds incubated in complete darkness, animal scientists Gregory Archer and Joy Mench report in January in Applied Animal Behaviour Science.
Chickens exposed to lots of light as eggs “would sit in the closest part of the box to me and just chill out,” Archer says. The others spent their time trying to get away. How light has its effect is unclear. On commercial chicken farms, eggs typically sit in warm, dark incubation rooms. The researchers are now testing light’s effects in large, commercial incubators. Using light exposure to raise less-fearful chickens could reduce broken bones during handling at processing plants, Archer says. It might also decrease harmful anxious behaviors, such as feather pecking of nearby chickens.
Babies are born germy, and that’s a good thing. Our microbiomes — the microbes that live on and in us — are gaining cred as tiny but powerful keepers of our health.
As microbes gain scientific stature, some scientists are trying to answer questions about how and when those germs first show up on babies. Birth itself may be an important microbe-delivery event, some researchers suspect. A trip through the birth canal can coat a baby with bacteria from his mother. A C-section, some evidence suggests, might introduce different bacteria, at least right after birth.
That difference forms the basis of the practice of vaginal seeding, which involves wiping vaginal fluids onto a baby born by C-section to introduce microbes the baby would have encountered in a vaginal birth.
Even while some parents are asking for the procedure, there’s dissent in the ranks of research about its benefits. Scientists don’t agree yet on how — or even whether — type of birth affects the microbiome. “It’s murky,” says obstetrician and maternal-fetal medicine specialist Kjersti Aagaard of the Baylor College of Medicine in Houston. Existing studies don’t clearly distinguish the effects of the C-section itself from those of certain diseases or conditions that can make a C-section more likely, such as maternal diabetes or obesity, she says. Other issues, like whether a baby received antibiotics or is breastfed, also muddy the waters. “You are left saying, ‘Wait a minute. Is it the surgery or not the surgery? What’s going on here?’” Aagaard says.
In a search for clarity, Aagaard and her colleagues surveyed the microbiomes of 81 pregnant women. Later on, the researchers added a second group of 82 women, whose microbiomes were assessed at the birth of their children.
Just after birth, babies who had been delivered by C-section had different mouth, nose and skin microbiomes than babies born vaginally. One possible explanation is that these babies are handled differently just after birth, Aagaard says. The microbiomes of the babies’ meconium, or stool, appeared to be similar, regardless of how the babies were born.
But between four and six weeks later, these C-section/vaginal birth differences on the mouth, nose and skin were largely gone, Aagaard says. The microbes living in and on the babies born by C-section and those born vaginally were nearly indistinguishable, the researchers reported online January 23 in Nature Medicine. Depending on where they lived, the populations of microbes had already taken on distinct identities by about a month after birth, the researchers found. Communities of nose-dwelling microbes were easy to distinguish from those living in the gut, for instance. These regional differences are signs of surprising microbial maturity, Aagaard says. “Postnatal microbiomes start looking like adults a little sooner than we may have appreciated,” she says.
The results raise an interesting question: If the type of birth isn’t one of the main shapers of microbiomes, then how and when do microbes get into babies? It’s possible that microbes from mothers slip into fetuses during pregnancy — a plausible idea, given some earlier results. Genetically tagged bacteria fed to pregnant mice showed up in their fetuses’ guts a day before the predicted due date, a result that suggests the bacteria traveled from mother to fetus. And Aagaard and colleagues have found evidence of microbes in the placenta of human mothers. They are now studying whether microbes, or perhaps pieces of them, move through the placenta from mother to baby. If that turns out to be the case, then babies meet their microbes, for better or worse, well before their birthday.
Every summer, people flock to the Great Lakes to swim and fish in the seemingly infinite waters and hike along the idyllic shores. But an ominous undercurrent flows just out of sight. Below the water’s surface rages an environmental catastrophe 200 years in the making.
In The Death and Life of the Great Lakes, journalist Dan Egan describes how the lakes’ natural history gave way to an unnatural one. From the effects of global trade and urbanization to climate change, the book offers an exhaustive (and sometimes exhausting) account of the abuses the lakes have endured. Scars left by retreating glaciers and a failed continental rift, lakes Huron, Ontario, Michigan, Erie and Superior are more like inland seas, holding about 20 percent of Earth’s surface freshwater. The lakes were mostly isolated from international waters until a series of canals and seaways let in freighters from around the world. “These ships are like syringes,” as one biologist put it, injecting into the lakes living pollution.
Nearly 200 nonnative species now call the lakes home. The worst offenders — alewives, sea lampreys and zebra and quagga mussels — have ruined food webs. Egan dedicates a third of the book to these invaders and biologists’ best, and sometimes misguided, efforts to contain them.
But the lakes also face lesser-known problems. Egan deftly explains the science of these complex issues, including runoff-induced toxic algal blooms and extreme fluctuations in the lakes’ water levels attributed to climate change.
Despite all the bad news, there are glimmers of hope. After decades of living on the brink of collapse, native whitefish and trout are regaining a foothold — a boon for the ecosystem and local economies. Scientists are also experimenting in the lab with gene drives to stop invasive Asian carp and with new ways to rid ships of stowaways lurking in ballast water.
The lakes still face overwhelming challenges, but their biggest threat, Egan argues, is our own ignorance: “We are still treating the lakes … as liquid highways that promise a shortcut to unimaginable fortune.” With few easy solutions and numerous political roadblocks, future generations are “perhaps the best hope the lakes have to recover,” he writes. But if this book is any indication, there’s no time to wait.
Parasites can drive their hosts to do weird, dumb things. But in certain oak trees, the parasites themselves get played.
“Creepy and awesome,” says Kelly Weinersmith of Rice University in Houston, who has helped reveal a Russian doll of nested parasitisms.
The saga begins when two majestic live oak species in the southeastern United States send out new shoots, and female crypt gall wasps (Bassettia pallida) arrive to lay eggs. A wasp mom uses the delivery end of her reproductive tract to drill through tree bark, injecting each of her eggs into a separate spot in the oak. Wasp biochemistry induces the tree to form a botanical womb with an edible lining largely free of oak defense chemicals. The tree is hijacked into nurturing each larva, and wasp life is good — until the unlucky ones get noticed by a second exploiter.
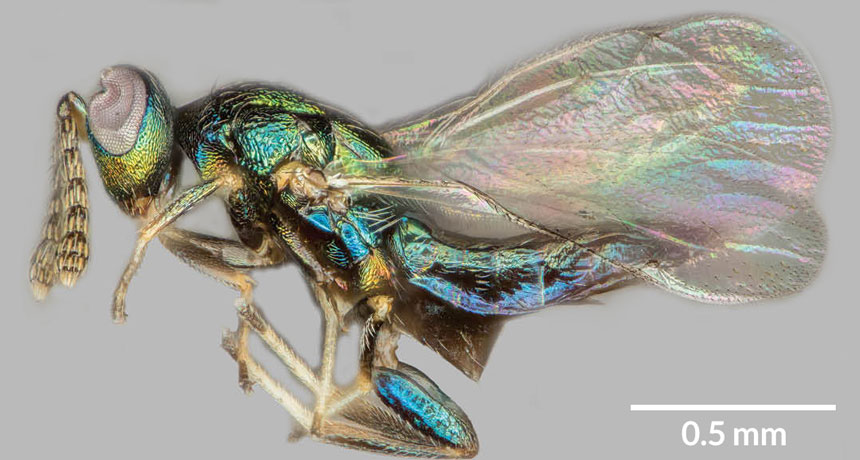
Another wasp species, a newly discovered Euderus, arrives, barely visible to the naked eye but “amazingly iridescent,” Weinersmith says. Her colleague at Rice, Scott Egan, named these jewel blue and green specks after Set, an Egyptian god of evil and chaos. E. set wasps enslave the B. pallida as laborers and living baby food. E. set females sense their prey inside the gall and inject eggs that hatch and feed on the original occupant. When the invaders mature, they are typically too frail to dig themselves out of the tree.But that’s not a problem, Weinersmith, Egan and colleagues report in the Jan. 25 Proceedings of the Royal Society B. That’s because, despite having a gnawing parasite inside, B. pallida wasps dig a tunnel to freedom.
Almost. When infested with E. set, the tunnelers don’t manage a large enough hole for their own escape. They die with their heads plugging the tunnel exit, perfect for the E. set attackers, who chew an escape hole through the stuck noggins.
Weinersmith and Egan may be the first to describe E. set’s manipulation, but what could be a much earlier example was collected by Alfred Kinsey — yes, that Kinsey. Before shocking mid-20th century America with explicit chronicles of human sexual behavior, he specialized in gall wasps.
Kinsey named more than 130 new species in just three years, collecting at least 5.5 million specimens, now at New York’s American Museum of Natural History. One of his Bassettia has its head stuck in a too-small exit hole in a stem, suggesting a chaos-and-death wasp lurks inside.
Scientists have long sought a strategy for curing genetic diseases, but — with just a few notable exceptions — have succeeded only in their dreams. Now, though, researchers in China and Texas have taken a step toward making the fantasies a reality for all inherited diseases.
Using the gene-editing tool known as CRISPR/Cas9, the researchers have successfully edited disease-causing mutations out of viable human embryos. Other Chinese groups had previously reported editing human embryos that could not develop into a baby because they carried extra chromosomes, but this is the first report involving viable embryos (SN Online: 4/8/16; SN Online: 4/23/15). In the new work, reported March 1 in Molecular Genetics and Genomics, Jianqiao Liu of Guangzhou Medical University in China and colleagues used embryos with a normal number of chromosomes. The embryos were created using eggs and sperm left over from in vitro fertilization treatments. In theory, the embryos could develop into a baby if implanted into a woman’s uterus.
Researchers in Sweden and England are also conducting gene-editing experiments on viable human embryos (SN: 10/29/16, p. 15), but those groups have not yet reported results.
Human germline editing wasn’t realistic until CRISPR/Cas9 and other new gene editors came along, says R. Alta Charo, a bioethicist at the University of Wisconsin Law School in Madison. “We’ve now gotten to the point where it’s possible to imagine a day when it would be safe enough” to be feasible. Charo was among the experts on a National Academies of Sciences and Medicine panel that in February issued an assessment of human gene editing. Altering human embryos, eggs, sperm or the cells that produce eggs and sperm would be permissible, provided there were no other alternatives and the experiments met other strict criteria, the panel concluded (SN: 3/18/17, p. 7). Still, technical hurdles remain before CRISPR/Cas9 can cross into widespread use in treating patients.
CRISPR/Cas9 comes in two parts: a DNA-cutting enzyme called Cas9, and a “guide RNA” that directs Cas9 to cut at a specified location in DNA. Guide RNAs work a little like a GPS system, says David Edgell, a molecular biologist at Western University in London, Ontario. Given precise coordinates or a truly unique address, a good GPS should take you to the right place every time.
Scientists design guide RNAs so that they will carry Cas9 to only one stretch of about 20 bases (the information-carrying subunits of DNA) out of the entire 6 billion base pairs that make up the human genetic instruction book, or genome. But most 20-base locations in the human genome aren’t particularly distinctive. They are like Starbucks coffee shops: There are a lot of them and they are often similar enough that a GPS might get confused about which one you want to go to, says Edgell. Similarly, guide RNAs sometimes direct Cas9 to cut alternative, or “off-target,” sites that are a base or two different from the intended destination. Off-target cutting is a problem because such edits might damage or change genes in unexpected ways.
“It’s a major issue for sure,” says Bruce Korf, a geneticist at the University of Alabama at Birmingham and president of the American College of Medical Genetics and Genomics Foundation. Doctors trying to correct one genetic defect in a patient want to be sure they aren’t accidentally introducing another.
But CRISPR/Cas9’s propensity to cut undesired sites may be exaggerated, says Alasdair MacKenzie, a molecular biologist at the University of Aberdeen in Scotland. In experiments with mice, MacKenzie and colleagues limited how much Cas9 was produced in cells and made sure the enzyme didn’t stick around after it made an edit. No off-target cuts were detected in any of the mice resulting from successfully edited embryos, MacKenzie and colleagues reported in November in Neuropeptides.
Other researchers have experimented with assembling the Cas9 and guide RNAs outside of the cell and then putting the preassembled protein-RNA complex into cells. That’s the strategy the Chinese researchers took in the new human embryo–editing study. No off-target cuts were detected in that study either, although only one edited embryo was closely examined.
Other researchers have been tinkering with the genetic scissors to produce high-fidelity versions of Cas9 that are far less likely to cut at off-target sites in the first place.
When a guide RNA leads Cas9 to a site that isn’t a perfect match, the enzyme can latch onto DNA’s phosphate backbone and stabilize itself enough to make a cut, says Benjamin Kleinstiver, a biochemist in J. Keith Joung’s lab at Harvard Medical School. By tweaking Cas9, Kleinstiver and colleagues essentially eliminated the enzyme’s ability to hold on at off-target sites, without greatly harming its on-target cutting ability.
Regular versions of Cas9 cut between two and 25 off-target sites for seven guide RNAs the researchers tested. But the high-fidelity Cas9 worked nearly flawlessly for those guides. For instance, high-fidelity Cas9 reduced off-target cutting from 25 sites to just one for one of the guide RNAs, the researchers reported in January 2016 in Nature. That single stray snip, however, could be a problem if the technology were to be used in patients. A group led by CRISPR/Cas9 pioneer Feng Zhang of the Broad Institute of MIT and Harvard tinkered with different parts of the Cas9 enzyme. That team also produced a cutter that rarely cleaved DNA at off-target sites, the team reported last year in Science.
Another problem for gene editing has been that it is good at disabling, or “knocking out,” genes that are causing a problem but not at replacing genes that have gone bad. Knocking out a gene is easy because all Cas9 has to do is cut the DNA. Cells generally respond by gluing the cut ends back together. But, like pieces of a broken vase, they rarely fit perfectly again. Small flaws introduced in the regluing can cause the problem gene to produce nonfunctional proteins. Knocking out genes may help fight Huntington’s disease and other genetic disorders caused by single, rogue versions of genes.
Many genetic diseases, such as cystic fibrosis or Tay-Sachs, are caused when people inherit two mutated, nonfunctional copies of the same gene. Knocking those genes out won’t help. Instead, researchers need to insert undamaged versions of the genes to restore health. Inserting a gene starts with cutting the DNA, but instead of gluing the cut ends together, cells use a matching piece of DNA as a template to repair the damage.
In the new human embryo work, Liu and colleagues, including Wei-Hua Wang of the Houston Fertility Institute in Texas, first tested this type of repair on embryos with an extra set of chromosomes. Efficiency was low; about 10 to 20 percent of embryos contained the desired edits. Researchers had previously argued that extra chromosomes could interfere with the editing process, so Liu’s group also made embryos with the normal two copies of each chromosome (one from the father and one from the mother). Sperm from men that have genetic diseases common in China were used to fertilize eggs. In one experiment, Liu’s group made 10 embryos, two of which carried a mutation in the G6PD gene. Mutations in that gene can lead to a type of anemia.
Then the team injected Cas9 protein already leashed to its guide RNA, along with a separate piece of DNA that embryos could use as a template for repairing the mutant gene. G6PD mutations were repaired in both embryos. Since both of the two embryos had the repair, the researchers say they achieved 100 percent efficiency. But one embryo was a mosaic: It carried the fix in some but not all of its cells. Another experiment to repair mutations in the HBB gene, linked to blood disorders, worked with 50 percent efficiency, but with some other technical glitches.
Scientists don’t know whether editing just some cells in an embryo will be enough to cure genetic diseases. For that reason, some researchers think it may be necessary to step back from embryos to edit the precursor cells that produce eggs and sperm, says Harvard University geneticist George Church. Precursor cells can produce many copies of themselves, so some could be tested to ensure that proper edits have been made with no off-target mutations. Properly edited cells would then be coaxed into forming sperm or eggs in lab dishes. Researchers have already succeeded in making viable sperm and eggs from reprogrammed mouse stem cells (SN: 11/12/16, p. 6). Precursors of human sperm and eggs have also been grown in lab dishes (SN Online: 12/24/14), but researchers have yet to report making viable human embryos from such cells.
The technology to reliably and safely edit human germline cells will probably require several more years of development, researchers say.
Germline editing — as altering embryos, eggs and sperm or their precursors is known — probably won’t be the first way CRISPR/Cas9 is used to tackle genetic diseases. Doctors are already planning experiments to edit genes in body cells of patients. Those experiments come with fewer ethical questions but have their own hurdles, researchers say.
“We still have a few years to go,” says MacKenzie, “but I’ve never been so hopeful as I am now of the capacity of this technology to change people’s lives.”